Esophageal and gastric cancer surgery
Esophageal cancer
Esophageal cancer is a cancer located in the esophagus. The two main sub-types of the disease are esophageal squamous-cell carcinoma (ESCC) and esophageal adenocarcinoma (EAC). Esophageal adenocarcinoma (EAC) is one of the most rapidly increasing tumor entities in the Western world. Over the past decades, the incidence of esophageal squamous cell carcinoma has decreased significantly in the U.S. and Europe. At the same time, the incidence of adenocarcinoma (EAC) has increased rapidly, especially among men. Risk factor for the squamous-cell type include tobacco, alcohol, very hot drinks and poor diet. The most common causes of the adenocarcinoma type are smoking tobacco, obesity, and acid reflux.
What are the symptoms of esophageal cancer?
In the beginning of the disease, esophageal carcinoma often remains asymptomatic. Symptoms usually appear after the cancer has infiltrated a larger part of the esophagus and caused stenosis. The first and the most common symptom is usually difficulty in swallowing, which is often experienced first with solid foods and later with softer foods and liquids. Eventual weight loss due to reduced appetite and undernutrition is common. Some patient experience pain while swallowing or pain behind the breastbone or stomach.
How is esophageal cancer diagnosed?
The diagnosis is made with an endoscopy and biopsy of suspicious lesions. After the diagnosis of esophageal cancer, further testing is needed to assess how much the cancer has spread. Esophageal endoscopic ultrasound can provide staging information regarding the level of tumor invasion, and possible spread to regional lymph nodes. Computed tomography (CT) can evaluate whether the cancer has spread to distant organs. Positron emission tomography is sometimes used if the CT scan results are inconclusive.
How is esophageal cancer treated?
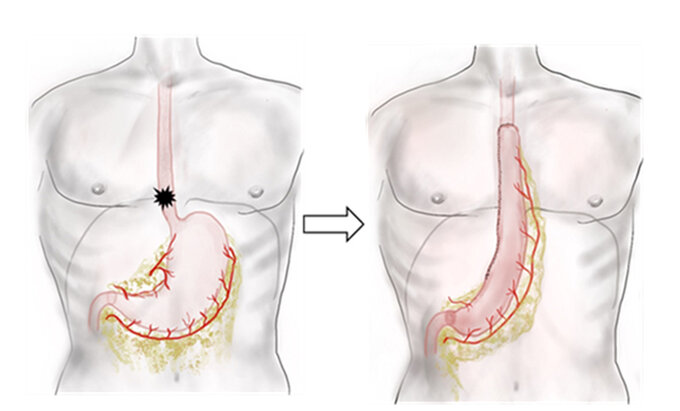
A multidisciplinary team covering various specialties manages the cancer treatment. All patients are discussed in our multidisciplinary tumor board, where the decision for treatment strategy is been made. Depending of the sub-type, tumorstage and lymph node involvement, usually patients undergo a perioperative chemotherapy or neoadjuvant chemoradiation. After this treatment, surgery is needed to remove the cancer. In cases of small esophageal cancers without lymph node involvement, treatment can consist of surgery only. The operation needed to remove the esophageal cancer is called esophagectomy. During esophagectomy, the part of the esophagus that contains the cancer and nearby lymph nodes are removed as well as the upper part of the stomach. The remaining esophagus is reconnected to the remaining part of the stomach. To do this the stomach is being pulled up in the thoracic cavity and connected to the remaining esophagus. At the Medical Centre of the University of Freiburg, the gold standard technique for esophageal resections is the hybrid minimally invasive esophagectomy (HMIE) as highly standardized procedures. In HMIE the abdominal part of the operation is done by a minimally invasive laparoscopic approach. The mediastinal resection plus reconstruction is performed by a thoracic approach through a muscle-sparing thoracotomy on the right side.
Gastric cancer
Gastric cancer, which is also known as gastric cancer, is a cancer that starts in the stomach. The exact location of the cancer in the stomach my impact the surgery neaded. The prognosis for people with small stomach cancers is quite good. Most stomach cancers are found when the disease is advanced and a cure becomes less likely. The cancer may spread from the stomach to other parts of the body, particularly the liver, lungs, bones, lining of the abdomen, and lymph nodes. Globally, stomach cancer is the fifth-leading type of cancer and the third-leading cause of death from cancer. The rates of gastric cancer have sharply declined among younger generations in the West, while they remain high for people living in East Asia.
What are the symptoms of gastric cancer?
In the beginning of the disease, gastric cancer often remains asymptomatic. When symptoms appear, they can include indigestion and pain in the upper part of the belly. Eventual weight loss due to reduced appetite and undernutrition is common, as well as as feeling very tired. In later stages of the cancer vomiting blood and black stools may appear.
How is gastric cancer diagnosed?
The diagnosis is made with an endoscopy and biopsy of suspicious lesions. After the diagnosis of gastric cancer, further testing is needed to assess how much the cancer has spread. Gastric endoscopic ultrasound can provide staging information regarding the level of tumor invasion, and possible spread to regional lymph nodes. Computed tomography (CT) can evaluate whether the cancer has spread to distant organs. Positron emission tomography is sometimes used if the CT scan results are inconclusive. Sometimes imaging tests don't give a clear picture of the cancer, so surgery is needed to see inside the body. With a minimally invasive surgery, we can look for small cancer spread in the belly.
How is gastric cancer treated?
A multidisciplinary team covering various specialties manages the cancer treatment. All patients are discussed in our multidisciplinary tumor board, where the decision for treatment strategy is been made. Depending of the sub-type, tumorstage and lymph node involvement, usually patients undergo a perioperative chemotherapy. After this treatment, surgery is needed to remove the cancer. In case of very small gastric cancers without lymph node involvement, treatment can consist of surgery only. The extend of the operation needed to remove the gastric cancer depends on the exact localisation of the cancer in the stomach. In some cases the cancer can be removed by resection of part of the stomach. This procedure is called a subtotal gastrectomy. In some cases, the entire stomach needs to be removed. This procedure is called a total gastrectomy. In both cases, the removed part or the whole stomach will be replaced with parts of the small intestine. These operations are done minimally invasive and leave only small scars. After recovery of the operation you will be able to eat everything but in small portions. Patients usually need 6-8 small meals each day after a gastrectomy.
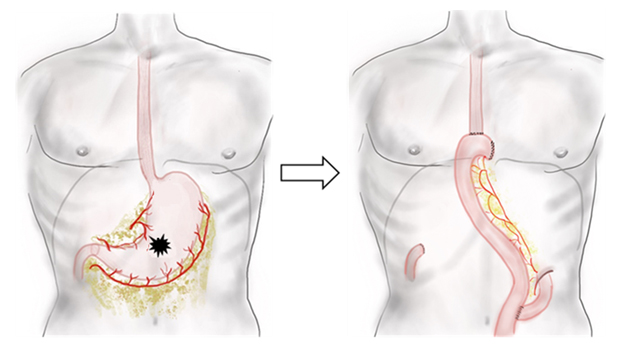
Fig.: Total gastrectomy