Deep brain stimulation (DBS)
©UKF
The deep brain stimulation (DBS) procedure has been established for more than 30 years and there is worldwide experience with the treatment of Parkinson's disease, tremors, dystonia, epilepsy, neuropathic pain, and other indications.
DBS is an essential part of the treatment of various neurological diseases in which conservative and drug therapy is no longer effective or leads to side effects.
WHAT IS DEEP BRAIN STIMULATION (DBS)?
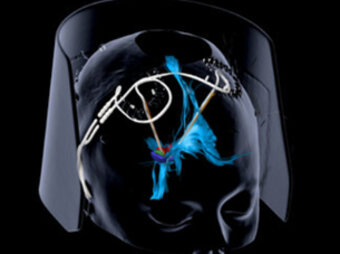
Deep brain stimulation (DBS) is a neurosurgical procedure in which thin electrodes are precisely inserted into specific areas of the brain. These electrodes are connected to a pulse generator (neurostimulator) which, similar to a pacemaker, is placed under the skin (usually below the collarbone). The device sends weak electrical impulses to the target areas in the brain to modulate activity in these regions. The pulse generator contains the battery and electronics to control the impulses.
HOW DOES DBS WORK?
The electrical impulses influence the activity of the nerve cells in the target areas. They can calm overactive nerve cells or stimulate underactive ones, thereby normalizing disturbed networks in the brain. The stimulation parameters (frequency, pulse duration, voltage) are individually adjusted to achieve the best effect for the patient.
CLINICAL PICTURES AND TARGET AREAS
If certain diseases can no longer be adequately treated with medication or if these medications cause intolerable side effects, DBS may be an option.
PARKINSON'S DISEASE
Parkinson's disease is a progressive neurodegenerative disorder caused by the loss of nerve cells in the brain that produce the neurotransmitter dopamine. The classic symptoms are tremors, muscle stiffness (rigidity), slowed movements (bradykinesia), and postural instability. In advanced stages,
many patients suffer from severe fluctuations in their mobility (known as ON-OFF fluctuations) and involuntary movements (dyskinesia) despite optimized drug therapy.
DBS therapy is considered for Parkinson's patients who generally still respond well to drug therapy with L-dopa but suffer from significant fluctuations, dyskinesia, or other side effects.
A type-specific diagnosis and an age of onset below 70 years are essential for successful treatment with this method.
TARGET AREAS IN PARKINSON'S DISEASE:
1. SUBTHALAMIC NUCLEUS (STN):
- The most commonly selected target area in Parkinson's disease
- Most commonly used in cases of fluctuation in efficacy
- Particularly effective against all cardinal symptoms (tremor, rigidity, bradykinesia)
- Often enables a significant reduction in medication dosage (30-60%)
- May occasionally cause mood swings or cognitive changes
2. GLOBUS PALLIDUS INTERNUS (GPI):
- Particularly effective against dyskinesia
- Less potential for medication reduction compared to STN
- Lower risk of psychiatric side effects
- Preferred for older patients or those with existing cognitive impairments
3. VENTRAL INTERMEDIATE THALAMIC NUCLEUS (VIM):
- Mainly effective against tremors
- Less effective on other Parkinson's symptoms
- Less commonly used today, except in patients with tremor-dominant Parkinson's
- Can also be used for essential tremor
The target area is selected on an individual basis, taking into account the dominant symptoms, age, cognitive abilities, and other patient-specific factors. DBS can significantly improve quality of life by reducing motor symptoms by an average of 60-70% and reducing treatment-related complications.
ESSENTIAL TREMOR
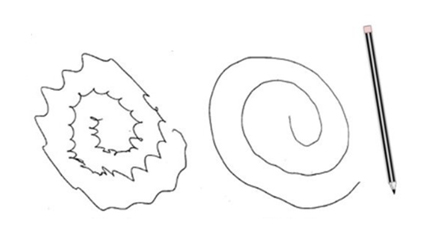
Fig. 1. Typical therapeutic effect on tremor under treatment with DBS
Essential tremor is the most common movement disorder and affects around 4-5% of the population over the age of 65. Unlike Parkinson's tremor, it typically occurs during movement or when holding a position (postural and action tremor) and improves at rest. The hands are most commonly affected, but the head, voice, tongue, and other parts of the body can also be affected. The disease often runs in families and is frequently hereditary. Patients often notice an improvement even when consuming small amounts of alcohol.
Essential tremor can be very stressful and significantly impair everyday activities such as eating, drinking, writing, or fine handiwork. Many patients also experience social isolation due to feelings of shame. Drug therapy with propranolol (a beta blocker) or primidone (an antiepileptic) is effective in about 50% of patients, but often wears off over time or causes unwanted side effects.
DBS is a particularly effective option for drug-resistant essential tremor. The main target is the ventral intermediate nucleus of the thalamus (Vim). Stimulation can reduce tremors by 80-90%, leading to a significant improvement in quality of life. The effect usually lasts for many years, but may diminish over time in some patients (habituation). Typical candidates for DBS are patients with severe, disabling tremor that does not respond adequately to medication and significantly restricts their daily lives. Age plays a lesser role than in Parkinson's disease, as long as the patient's general health allows surgery.
DYSTONIA
Dystonia is a neurological movement disorder characterized by persistent or recurrent muscle contractions. These lead to involuntary rotational movements, abnormal postures, or repetitive movements. Dystonia can affect a single part of the body (focal dystonia), several adjacent parts of the body (segmental dystonia), or the entire body (generalized dystonia).
EXAMPLES OF FOCAL DYSTONIA INCLUDE:
- Cervical dystonia (torticollis): twisting of the neck and/or head
- Blepharospasm: involuntary closing of the eyes
- Oromandibular dystonia: jaw and facial spasms
- Writer's cramp: cramping of the hand when writing
Primary dystonia is often genetic, with the DYT1 gene mutation being the most common cause of early-onset generalized dystonia. Symptoms often begin in childhood or adolescence in one part of the body and then spread.
DBS has proven to be an effective treatment option for severe, drug-resistant dystonia. The internal globus pallidus (GPi) is the preferred target area. In contrast to Parkinson's disease or essential tremor, the full effect of DBS in dystonia often only becomes apparent after weeks or months, as the neural networks reorganize more slowly. The prospects of success are particularly good in primary generalized or segmental dystonia with DYT1 mutation (improvement of 60-90%). In focal dystonia, treatment with botulinum toxin is usually attempted first before DBS is considered.
SECONDARY DYSTONIA
Secondary dystonia differs from primary dystonia in that it is caused by identifiable factors such as brain injury, stroke, oxygen deprivation during birth, infection, certain medications, or metabolic disorders. The most common form is cerebral movement disorder following early childhood brain damage. The clinical picture is often more complex than in primary dystonia and may be combined with other movement disorders such as spasticity, chorea, or athetosis.
Symptoms can change significantly throughout the day and be exacerbated by fatigue, stress, or certain body positions. DBS for secondary dystonia is more complicated and the results are less predictable than for primary forms. Success depends heavily on the underlying disease, the age at onset, and the duration of the disease. In dystonic cerebral palsy, improvements in motor functions of 20-30% can be achieved, while tardive dystonia (drug-induced) responds better to DBS with improvements of 50-70%.
The globus pallidus internus (GPi) is also the preferred target area here. In patients with secondary dystonia, particularly careful patient selection and counseling are important in order to create realistic expectations. Often, the focus is on improving the care situation and reducing pain, rather than on complete restoration of function.
FOCAL EPILEPSY
We usually treat epilepsy in collaboration with the treatment team at the epilepsy center. Regular outpatient check-ups are also necessary in this case. Epilepsy is a chronic neurological disorder characterized by recurrent, unprovoked epileptic seizures. These seizures are caused by abnormal, synchronized electrical activity in the brain. Approximately 50 million people worldwide suffer from epilepsy, with the incidence statistically increasing in childhood and old age.
The standard treatment consists of antiepileptic drugs, which can control seizures in about 70% of patients. In drug-resistant epilepsy (persistent seizures despite adequate therapy with two different antiepileptic drugs), resective surgical procedures may be considered to remove the seizure-triggering focus.
DBS is used in patients with drug-resistant epilepsy in whom resection surgery is not possible because:
- the origin of the seizures cannot be reliably localized
- there are multiple seizure foci
- the seizure focus is located in a functionally important area
- previous surgeries have been unsuccessful
The anterior thalamic nucleus (ANT), the centromedian nucleus of the thalamus, the hippocampus, and the cerebellum have been established as target areas. The stimulation of the ANT has been particularly well studied, leading to a median seizure reduction of 56% after two years in the SANTE study, with approximately half of the patients achieving a seizure reduction of at least 50%.
The effect of DBS in epilepsy often develops slowly over months to years and may increase over time in some patients. Unlike in Parkinson's disease or essential tremor, immediate seizure control by switching on the stimulation is not to be expected. Antiepileptic medication is usually continued, but can often be reduced if the response is good.